(See Table 1.)
 Click on icon to see table/diagram/image
Molecular Formula:
Click on icon to see table/diagram/image
Molecular Formula: C
25H
34O
6.
Molecular Weight: 430.54 g/mol.
Excipients/Inactive Ingredients: Microcrystalline cellulose and carboxymethylcellulose sodium, Glucose anhydrous, Polysorbate 80, Disodium edetate, Potassium sorbate, Hydrochloric acid, Purified water.
Pharmacology: Pharmacodynamics: Budesonide is a corticosteroid with mainly glucocorticoid activity. It is used intranasally for the prophylaxis and treatment of allergic rhinitis. Corticosteroids are generally considered the most effective medications for the management of inflammatory diseases. Intranasal corticosteroids are quickly metabolized to less active metabolites, minimally absorbed, and have been associated with few systemic adverse effects. Studies have shown that control of allergic rhinitis symptoms by intranasal corticosteroids is dependent on local activity.
Glucocorticoid potency is closely related to their glucocorticoid receptor (GR) binding affinity within the target cell. This receptor binding triggers a cascade of biochemical reactions within the target cell, thereby affecting the rate of protein synthesis. This is responsible for the anti-inflammatory effect of glucocorticoids. Upon GR activation, there is a decrease in the production of cytokines and other inflammatory mediators such as kinins, histamine, and platelet activating factor. Corticosteroids also reduce the number of circulating T lymphocytes and inhibit activation of other T lymphocytes. The inhibition of T lymphocytes and cytokine production reduce the recruitment and influx of circulating eosinophils, macrophages, and basophils into the nasal epithelium.
Pharmacokinetics: Absorption: Budesonide is moderately lipophilic and systemic exposure is primarily due to its rapid absorption through the nasal mucosa. The systemic bioavailability of budesonide following intranasal administration is 6 to 16% while its pulmonary bioavailability is 28%.
Metered doses of budesonide 400 mcg to 1600 mcg given as single or repeated doses reach peak plasma concentrations of 0.51 nmol/L to 5.37 nmol/L and 2.03 nmol/L to 6.40 nmol/L, respectively. No consistent differences in the peak plasma concentrations between the epimers of budesonide, 22R and 22S, have been reported.
Following inhalation, the mean time to peak plasma concentration of budesonide is achieved within 1 to 2 hours.
Distribution: Budesonide is distributed widely into tissues with plasma protein binding averaging between 85 and 90%. The epimers of budesonide have large volumes of distribution - 424L for 22R-budesonide and 245 L for 22S-budesonide. 22R-budesonide has a larger volume of distribution than the 22S epimer due to its greater lipophilicity. At steady state, the active, unbound form of budesonide has a volume of distribution of approximately 3 L/kg in both adults and children.
Metabolism: Although budesonide is rapidly and extensively absorbed through the lungs, it is not biotransformed in the lung or gastrointestinal tract. Budesonide is metabolized in the liver primarily via oxidative and reductive pathways. Budesonide undergoes an extensive degree (~90%) of biotransformation on first passage by CYP3A4 enzymes to metabolites of low glucocorticosteroid activity. Major metabolites, 6β-hydroxybudesonide and 16α-hydroxyprednisolone, have similar half-lives but are relatively inactive compared to budesonide having less than 1% of its glucocorticoid and anti-inflammatory activity.
Elimination: Budesonide is excreted primarily as metabolites in the urine and feces. No intact budesonide has been detected in the urine. Budesonide systemic clearance is 0.92 to 1.4 L/min. The half-life of unchanged budesonide following both inhalation and intravenous administration averages between 2 to 4 hours.
Special Population: Pediatrics: The bioavailability of budesonide in children with asthma is reported to be 25.4±10.4% for the 22R epimer and 29.6±12.4% for the 22S epimer after inhalation of the nominal dose. Total systemic availability in 3- to 6-year old children is approximately 6% of the labeled dose and a peak plasma concentration of 2.6 nmol/L is achieved within 10 to 30 minutes after inhalation. The volume of distribution in children with asthma is reported at 3.11 kg/L and 4.8 kg/L for the 22R and 22S epimer of budesonide, respectively. At steady state, the volume of distribution has been reported to be 55 L when administered via nebulization. Systemic clearance is approximately 50% higher than in healthy adults. Total plasma clearance is higher for the 22R epimer than for the 22S epimer (2.0 L/kg·h versus 1.51 L/kg·h, P<0.001) while terminal elimination half-life is 2.3 hours.
Elderly: There are no budesonide pharmacokinetic data available in elderly patients.
Toxicology: Pre-Clinical Safety Data: Summary: Preclinical data reveal no special hazard for humans based on conventional studies of single and repeated dose toxicity, genotoxicity, carcinogenicity and toxicity to reproduction and development.
Relieves symptoms of seasonal or perennial allergic rhinitis (nasal congestion, runny nose, sneezing and itchy nose).
Treatment of allergic rhinoconjunctivitis (nasal congestion, runny nose, sneezing, itchy nose, itchy and watery eyes).
Prevention of allergic rhinitis.
Under the Supervision of a Healthcare Professional: Treatment of nasal polyps and prevention of nasal polyps after polypectomy.
Relieves symptoms of vasomotor rhinitis.
Some symptoms may get better on the first day of treatment. It may take up to two weeks of daily use to feel the most symptom relief.
For prevention, start therapy before anticipated exposure to the allergens.
64 mcg per spray Dose Formulation: Allergic Rhinitis and Vasomotor Rhinitis: Adults and Children 12 years and older: Once daily, use up to 2 sprays in each nostril (256 mcg total daily dose) while sniffing gently.
Once allergy symptoms improve, reduce dose to 1 spray in each nostril daily.
Children 6 years to less than 12 years of age: An adult should supervise use in children under age 12.
Once daily, use 1 spray in each nostril (total dose 128 mcg) while sniffing gently.
If symptoms do not improve, dose can be increased up to 2 sprays per nostril (up to 256 mcg total daily dose).
Once allergy symptoms improve, reduce dose to 1 spray in each nostril daily.
Talk to the child's physician if the child needs to use the spray for longer than two months a year.
Treatment and Prevention of Nasal Polyps: Adults and Children 12 years and older: Twice daily, use 1 spray in each nostril (256 mcg total daily dose) while sniffing gently.
No overdose-associated ADRs have been identified for budesonide nasal spray from review of the post-marketing safety data and from the literature.
Acute overdose with intranasal budesonide, even in excessive doses, is not expected to be a clinical problem.
Keep out of reach of children. In the event of overdose, get medical help or contact a Poison Control Center right away.
Hypersensitivity to budesonide or to any of the ingredients.
Systemic effects of nasal corticosteroids may occur, particularly at high doses prescribed for prolonged periods These effects are much less likely to occur than with oral corticosteroids and may vary in individual patients and between different corticosteroid preparations. Potential systemic effects may include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, cataract, glaucoma and more rarely, a range of psychological or behavioral effects including psychomotor hyperactivity, sleep disorders, anxiety, depression or aggression (particularly in children).
This product may slow the growth rate in some children when used in combination with other steroids.
Consult a physician before use if the patient is using a steroid medicine for conditions such as asthma, allergies or skin rash.
Consult a physician before use if the patient has ever been diagnosed with glaucoma, cataracts or an eye infection, or if the patient has diabetes.
Stop use and consult a physician if the patient has any change in vision.
Consult a physician before use if the patient has or has been exposed to someone who has tuberculosis, chicken pox or measles.
Consult a physician if the patient develops signs or symptoms of an infection such as persistent fever.
Consult a physician if the patient has severe or frequent nosebleeds, recent nose ulcers, nose surgery or has a nose injury that has not healed.
If symptoms persist or worsen, or if new symptoms occur, stop use and consult a physician.
Effects on Ability to Drive or Use Machines: There is no evidence that budesonide has an effect on the ability to drive or use machines.
There are no adequate well-controlled clinical studies in pregnant or breastfeeding women.
Pregnancy: It is not known if budesonide can cross the placenta but due to its relatively low molecular weight, placental transfer may be possible. When given at therapeutic doses, systemic exposure after intranasal administration is low.
Lactation: Budesonide is excreted in breast milk. However, due to negligible systemic exposure, minimal exposure to nasal budesonide in breast-fed infants is expected. The infant daily dose of inhaled budesonide is around 0.3% of the maternal daily dose. There is a linear relationship between budesonide concentration in plasma and breast milk, where concentration of budesonide in breast milk is less than plasma concentration.
Fertility: There is no evidence that intranasally administered budesonide has an effect on fertility.
This product should not be used during pregnancy or lactation unless the potential benefit of treatment to the mother outweighs the possible risks to the developing fetus or nursing infant. Ask a physician before use if you are pregnant or breastfeeding.
Clinical Trial Data: The safety of budesonide from clinical trial data is based on data from 15 placebo-controlled randomized studies in the treatment of allergic rhinitis.
The Tables 2 to 3 include adverse events that occurred where greater than one event was reported, and the incidence was greater than placebo and in 1% of patients or more. (See Table 2 and Table 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Post Marketing Data: Adverse drug reactions (ADRs) identified during Post-marketing experience with budesonide are included in Table 4.
The frequencies are provided according to the following convention: Very common ≥1/10; Common ≥1/100 and < 1/10; Uncommon ≥1/1,000 and <1/100; Rare ≥1/10,000 and <1/1,000; Very rare <1/10,000; Not known (cannot be estimated from the available data).
In Table 4, ADRs identified are presented by frequency category based on 1) incidence in adequately designed clinical trials or epidemiology studies, if available or 2) when incidence is unavailable, frequency category is listed as Not known. (See Table 4.)
Click on icon to see table/diagram/image
CYP3A4 Inhibitors: Concomitant use of inhaled budesonide and cytochrome P450 inhibitors particularly isoenzyme CYP3A4 (i.e., cobicistat-containing products, ketoconazole, ritonavir, atazanavir, clarithromycin, indinavir, itraconazole, nefazodone, nelfinavir, saquinavir, telithromycin, itraconazole) increases the concentration of budesonide in the plasma leading to increased risk of systemic side-effects such as Cushing's syndrome and adrenal suppression. If used, close monitoring of patients is advised for any systemic effects. Otherwise, the combination should be avoided unless the benefit outweighs the risk. Short term use (1 to 2 weeks) of ketoconazole concomitantly with budesonide is not associated with clinically significant drug interaction.
Instructions for Use, Handling and Disposal: UNLESS INSTRUCTED OTHERWISE, DO NOT DISPOSE OF UNUSED MEDICINES BY EMPTYING THEM INTO YOUR SINK, TOILET OR STORM DRAIN.
Read the information before using Rhinocort Aqua nasal spray. Follow the directions carefully.
Before using Rhinocort Aqua nasal spray for the first time shake the bottle and then pump several times (5-10 times) into the air, so that a uniform mist is obtained.
If not used daily the pump must be loaded again. After the first time it is sufficient to pump just once (1) into the air.
1. Blow your nose. Shake the bottle.
Remove the protective cap.
2. Hold the bottle.
3. Insert the tip into your nostril and pump the number of doses prescribed.
Administer the spray into the other nostril in the same way.
4. Replace the protective cap. Do not use Rhinocort Aqua nasal spray more often than prescribed.
Children: Children should only use Rhinocort Aqua nasal spray under supervision by an adult to ensure that the dose is correctly administered and that the dosage is according to the doctor's prescription.
Cleaning: Clean the upper plastic parts regularly. Remove the protective cap and lift off the white nasal applicator. Wash the plastic parts in warm water. Allow the plastic part to air-dry completely before replacing them.
Do not try to clean the nasal applicator by using a pin or sharp object.
Rhinocort Aqua nasal spray does not give immediate relief. Generally it will take a few days to achieve full effect. It is therefore very important that Rhinocort Aqua is used regularly.
Incompatibilities: Not applicable.
Do not store above 30°C. Do not freeze.
Shelf-Life: 2 years.
R01AD05 - budesonide ; Belongs to the class of topical corticosteroids used for prophylaxis and treatment of allergic rhinitis.
Rhinocort Aqua nasal spray 64 mcg
120 dose x 1's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image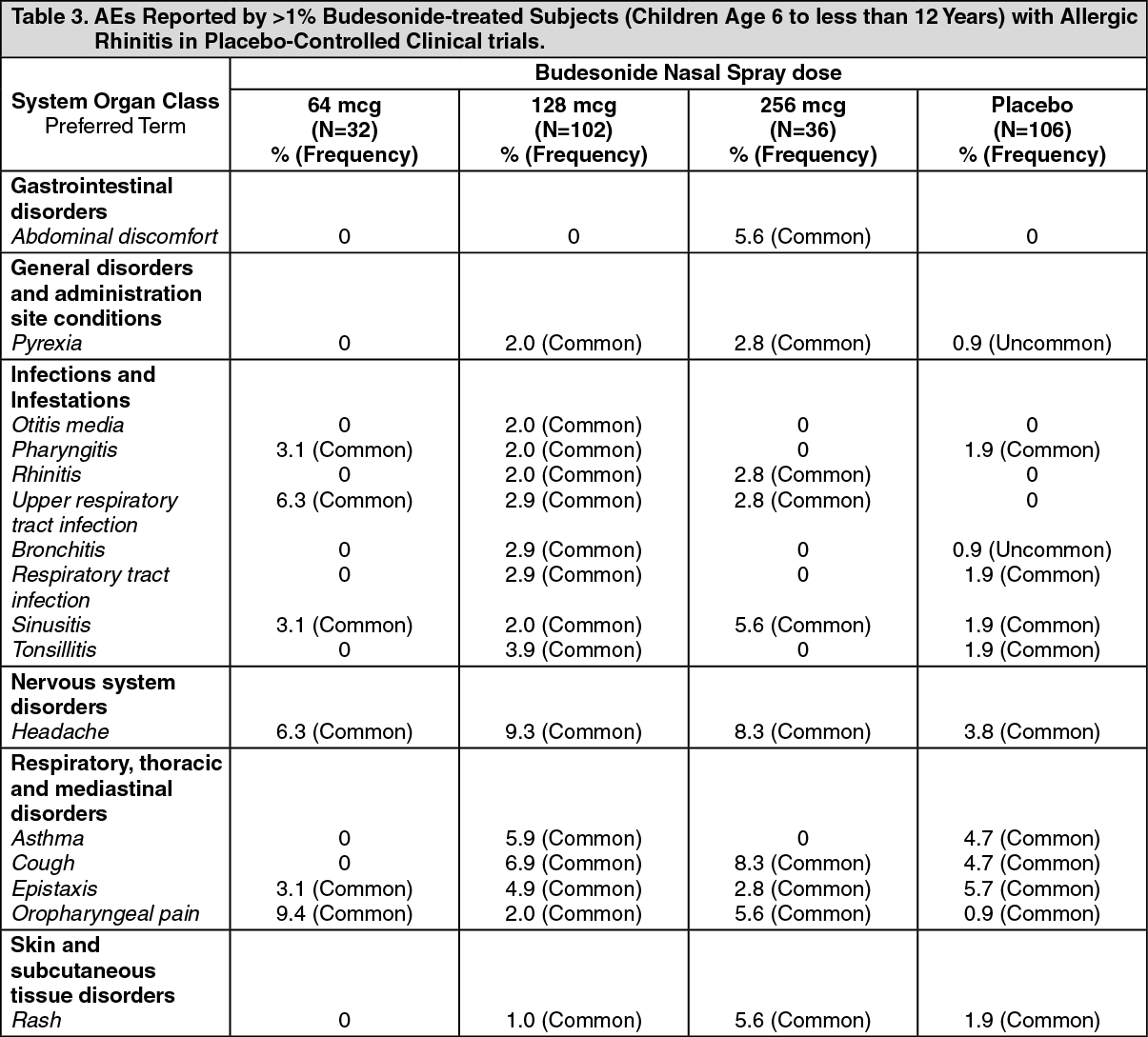 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image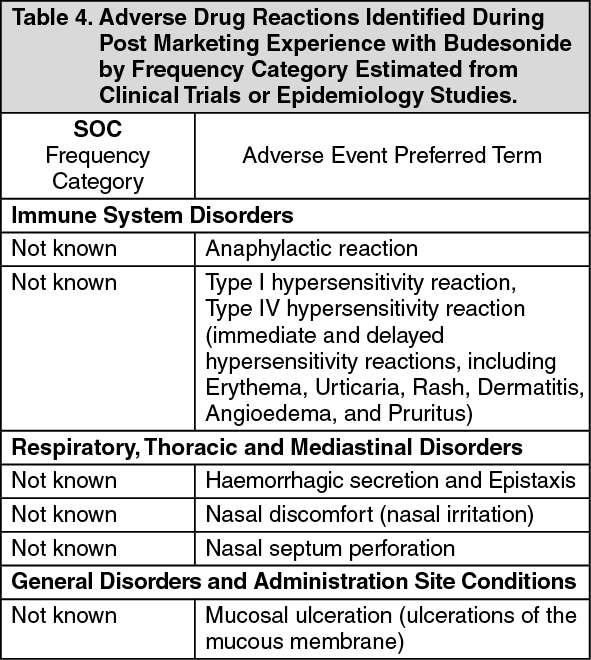 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
